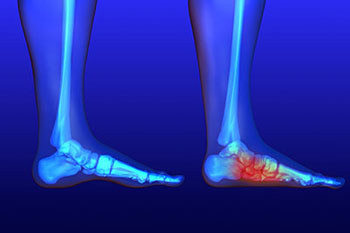
Flat feet is a condition that affects those who have little to no arch in their feet. When you stand, a person who doesn’t have flat feet will have a gap from the inner part of their feet to the floor, due to the normal arch that slightly rises off the ground. Those with flat feet will experience no such gap. While there are some people who experience no issues with their flat feet, it’s not uncommon for those with this condition to experience discomfort or pain.
Flat feet may cause a certain level of pain due to strained muscles and connecting ligaments. Those not afflicted by flat feet are able to get support while walking by the spring that the arch provides, which in turn, helps to distribute your body weight while taking steps. When the arch is no longer present, there is a larger amount of pressure on your muscles and ligaments in the feet, which is why they become strained and may cause you to feel pain.
There are many reasons that play a role in why a person may develop flat feet. For instance, certain genetic factors passed down from parents can lead to flat feet. Children may appear to have flat feet; however, their arches should develop over time. Having overall weak arches, a foot or ankle injury, arthritis, or a muscle or nervous system disease may all increase your likelihood of having flat feet. Tarsal coalition, a foot condition causing the fusion of bones in the feet, may also play a part in developing flat feet. Other common factors that are linked to flat feet include diabetes and obesity.
To manage the discomfort that may come with flat feet, we recommend that your practice exercises to help ease your pain. Heel cord stretches are a great way to stretch your Achilles tendon and help loosen up calf muscles that are often strained due to flat feet. Placing a golf ball under your foot and rolling it back and forth while seated is another great stretch, especially for your plantar fascia ligament.
When it comes to treating flat feet or fallen arches, it’s suggested you get plenty of rest. Frequently ice the affected area to help reduce swelling. Performing daily stretches are a great way to loosen up your muscles and relieve strain. It may also be beneficial to look into orthotics or shoe inserts to help relieve the pain.
If you’d like more information on how to treat discomfort you’re feeling because of flat feet, consult with a podiatrist for the best treatment options for your case.
